Living donor liver transplants are relatively uncommon in North America compared to Asia. Liver exchange might help change that. Here are some reports of recent and not so recent liver exchanges, including a non-simultaneous exchange chain at UCSF, and a simultaneous chain in Canada. Expect more in the near future.
(Non-simultaneous chains have become the backbone of kidney exchange in the U.S., so we may start to see longer chains of liver exchange as well.)
Here's the most recent report of a short non-directed donor chain:
Expanding living donor liver transplantation: Report of first US living donor liver transplant chain by Hillary J. Braun Ana M. Torres Finesse Louie Sandra D. Weinberg Sang‐Mo Kang Nancy L. Ascher John P. Roberts, American Journal of Transplantation, First published: 10 November 2020 https://doi.org/10.1111/ajt.16396
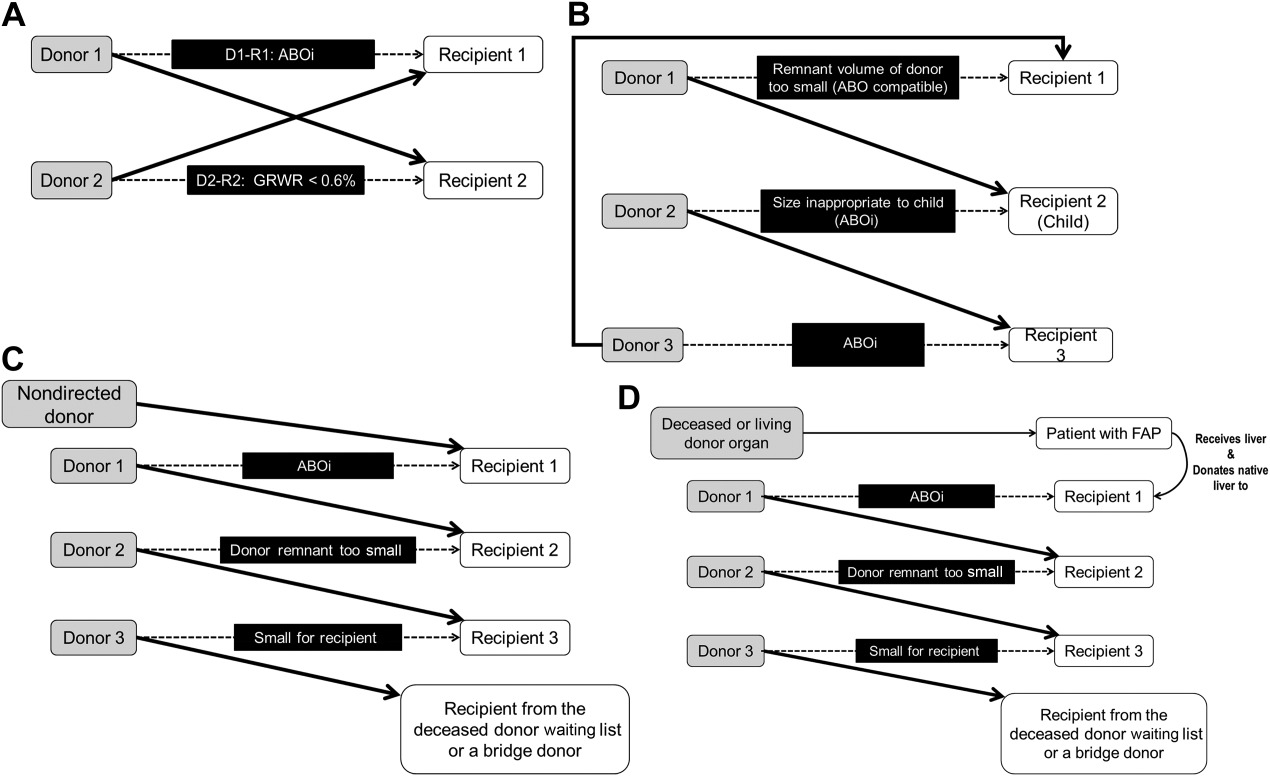
Abstract: "Living donor liver transplantation (LDLT) enjoys widespread use in Asia, but remains limited to a handful of centers in North America and comprises only 5% of liver transplants performed in the United States. In contrast, living donor kidney transplantation is used frequently in the United States, and has evolved to commonly include paired exchanges, particularly for ABO‐incompatible pairs. Liver paired exchange (LPE) has been utilized in Asia, and was recently reported in Canada; here we report the first LPE performed in the United States, and the first LPE to be performed on consecutive days. The LPE performed at our institution was initiated by a nondirected donor who enabled the exchange for an ABO‐incompatible pair, and the final recipient was selected from our deceased donor waitlist. The exchange was performed over the course of 2 consecutive days, and relied on the use and compliance of a bridge donor. Here, we show that LPE is feasible at centers with significant LDLT experience and affords an opportunity to expand LDLT in cases of ABO incompatibility or when nondirected donors arise. To our knowledge, this represents the first exchange of its kind in the United States."
The paper says this about the timing of the surgeries:
"Other centers reporting LPE have performed the donor and recipient operations in four operating rooms simultaneously4, 5 which can be logistically challenging, but addresses concerns regarding simultaneity and equalizing risk. In our case, we performed the operations on sequential days. In doing so, we accepted the risk that, given a good outcome in Recipient 1 on the first day, Donor 2 (the “bridge” donor) might opt out of living donation at the last moment. Reappropriating terminology from the kidney paired exchange (KPE) literature, a bridge donor is defined as someone who donates more than 1 day after their intended recipient received a transplant.12 A recent paper discussing the feasibility of LPE in the United States emphasized that, in the early days of KPE, there was concern that the bridge donor might back out at the last minute and break the chain.13 As a result, kidney donor operations were initially attempted simultaneously. However, a 2018 review of 344 KPE chains between 2008 and 2016 revealed that only 5.6% of bridge donors broke the chain and the majority of these donors developed a medical issue during their time as a bridge donor that prohibited them from completing donation.12 Ultimately, because this occurrence was so infrequent, the authors concluded that simultaneous donor operating rooms for chains are unnecessary and may actually deter potential donors based on logistical issues. "
***********
And here's a report from Canada of a non-directed donor chain of liver exchange with all surgeries conducted simultaneously (also with the NDD donating to an incompatible patient-donor pair whose donor donated to a patient on the deceased donor waiting list).
Living donor liver paired exchange: A North American first by Madhukar S. Patel Zubaida Mohamed Anand Ghanekar Gonzalo Sapisochin Ian McGilvray Blayne A. Sayed Trevor Reichman Markus Selzner Jed A. Gross Zita Galvin Mamatha Bhat Les Lilly Mark Cattral Nazia Selzner, American Journal of Transplantation, First published: 10 June 2020 https://doi.org/10.1111/ajt.16137
Abstract: Paired organ exchange can be used to circumvent living donor‐recipient ABO incompatibilities. Herein, we present the first case of successful liver paired exchange in North America. This 2‐way swap required 4 simultaneous operations: 2 living donor hepatectomies and 2 living donor liver transplants. A nondirected anonymous living donor gift initiated this domino exchange, alleviating an ABO incompatibility in the other donor‐recipient pair. With careful attention to ethical and logistical issues, paired liver exchange is a feasible option to expand the donor pool for incompatible living liver donor‐recipient pairs.
*******
Here's a 2014 report from S. Korea:
Section 16. Update on Experience in Paired-Exchange Donors in Living Donor Liver Transplantation For Adult Patients at ASAN Medical Center by Jung, Dong-Hwan1; Hwang, Shin1; Ahn, Chul-Soo1; Kim, Ki-Hun1; Moon, Deok-Bog1; Ha, Tae-Yong1; Song, Gi-Won1; Park, Gil-Chun1; Lee, Sung-Gyu, Transplantation: April 27, 2014 - Volume 97 - Issue - p S66-S69, doi: 10.1097/01.tp.0000446280.81922.bb
"Between January 2003 and December 2011, approximately 2,182 adult LDLT cases were included in this study. During this period, 26 paired-exchange donor LDLT cases were performed (1.2%).
"Results: Of the 26 paired-exchange donor LDLT cases, 22 pairs were matched due to ABO-incompatibility, and 4 pairs were matched because of cascade allocation of unrelated donors or relatively small graft volume to the recipients. A total of 28 living donors were included in the 26 paired-exchange donor LDLT cases because of inclusion of two dual-graft transplants. Elective surgery was performed in 22 cases, and urgent operation was performed in 4 cases. The overall 1-year and 5-year patient and graft survivals were both 96.2% and 90.1%, respectively.
"Conclusions : Our experience suggests that the paired-exchange donor program for adult LDLT seems to be a feasible modality to overcome donor ABO incompatibility."
**********
Here's a story of a liver exchange in Texas, between an incompatible pair and a compatible pair.
***********
Here's a liver exchange in Hong Kong between an incompatible pair and a compatible pair.
***********
Here's a report from two major liver transplant centers in Hong Kong and S. Korea. The Korean team reported 16 donor exchanges conducted over a 6-year period.