Last Tuesday, in Chile I was interviewed by Eduardo Olivares, the editor for Economics and Business of El Mercurio, which published the interview yesterday. We talked for an hour about market design generally, about how markets work when they're working well or working badly, and we spoke about school choice (where Chile is a leader) and transplantation (where it is not). The interview is behind a paywall, but below are some extracts (retranslated back into English via Google Translate).
On markets generally:
—Many people ask that “markets be free,” as has recently happened in Argentina. Should they be free?
“That's a complicated question. Markets should be free to function well, but they need conditions that allow them to function well. Having a free market does not necessarily mean a market without rules. A wheel can spin freely because it has a well-greased axle and bearings. A wheel by itself cannot turn very well, and the same goes for the market.”
—Who puts the oil in the wheel gears?
“That's the job of market design. Part of what makes markets work well are good market rules. The government has a role in regulating markets, concerning property rights and things like that. But on another level, entrepreneurs do things. Here in Santiago I [can]... call an Uber using the same app and rules I use in California. Uber is a marketplace for passengers and drivers. The rules can be made by both private organizations and the government.”
On prices:
—Do prices matter?
"A lot. “Prices are important to help allocate scarce resources, but also to make them less scarce.”
...
—When do they not matter?
“Let me start with when they matter a lot: in commodity markets. If you want to buy commodities, price is really the only thing that's happening. But when 'El Mercurio' wants to hire journalists, it doesn't limit itself to offering a salary: it wants it to be a good job, with special reporters. Price is important, but in other markets other things are also important. When you get a new job, the first question your friends ask you is not what the salary is, but who you work for.”
On school choice:
“Most markets are not commodity markets... In some markets we don't like prices to work at all. One of the places where Chile is a leader in market design is school choice: how people are assigned to schools and Chile has done a lot of work on this, although mainly for public schools.”
—What do you know about this system in Chile?
“Not long ago, before there was centralized and widespread school choice in Chile, there were the usual problems with decentralized school choice; That is, parents had to get up early to get in line, and they had a difficult process to register their children.”
—The new system has been criticized. Some claim it caused more people to choose the private system over the public school system. Isn't it similar to what is happening in New York, for example?
“There is something to that. In New York and Boston we also have a system that we call charter schools: free access schools, but organized by private entities, even if they are municipal schools. And they also have different standards. School choice is important, but it does not solve the problems of poverty or income inequality. Now, one of the reasons we have school choice in the United States and perhaps also in Chile is because we think that, otherwise, there is a danger that the poor will be condemned to send their children to poor schools. .
—Has there been any successful case in which parents can honestly rank the order of preference for the school they want their children to go to?
“In Chile, procedures are used that [make it] what game theorists call a dominant strategy to express true preferences. The [remaining] problem is not in creating systems that make it safe to express preferences, but in distributing the information so that people can form preferences sensibly. In the United States, the hardest families to reach are those who don't speak English at home, so it's sometimes difficult to communicate with them. And different families have different feelings about what kind of schools their children should attend.”
“The benefits of school choice come from the fact that some schools may be high quality for some children but not for others, so we would like children to attend the schools that are best quality for them.”
On kidneys:
—You are famous for the proposal that allowed the “kidney exchange.” Years after the first experience, what do you see now in this type of market?
“Kidney exchange is working quite well in the US, but it works especially well for patients who are not too difficult to match. Even in the US, a fairly large country, we have patients who are so difficult to match that we have trouble finding a kidney for them.”
—And in other countries?
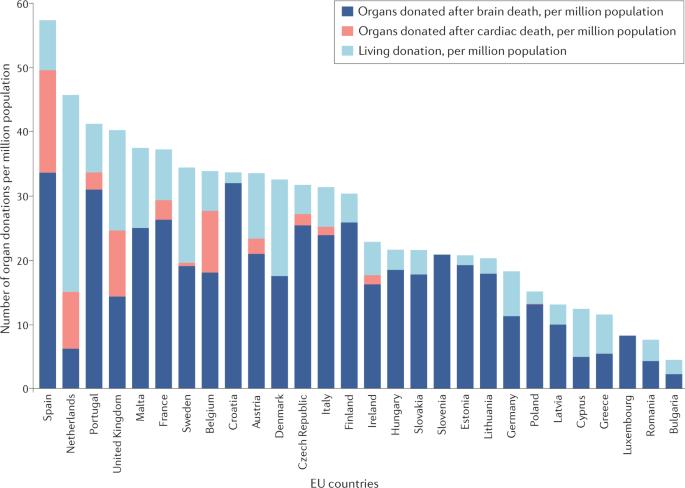
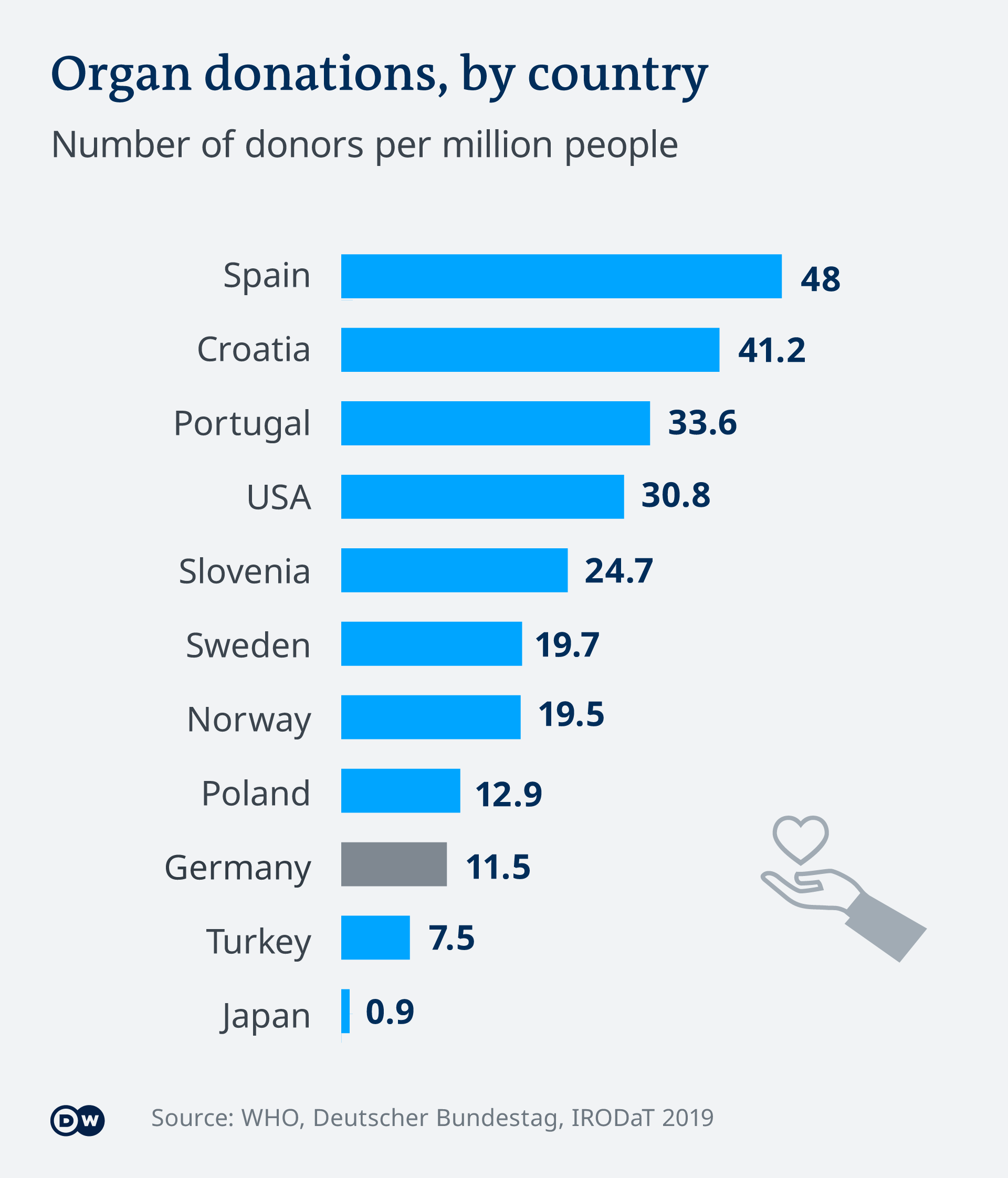
“Smaller countries, with 20 million inhabitants, like Chile, would benefit if we could make national borders not so important. When we look at transplants per million inhabitants, Chile is in the middle of the world. But since it is a small country, when the total number of transplants performed is analyzed, Chile has very few. Kidneys are obtained from both deceased and living donors. In Chile, as in much of the world, the majority of transplants come from deceased donors. Kidney exchange would allow more transplants to come from living donors ... “Twenty million is not enough, so it would be very good to see in South America an exchange of kidneys that can cross between countries, which is not so easy to do.”
Equality of exchange and the role of perceptions
“One of the things that worries people when talking about transplants is that [they think it might be] a medical process that exploits the poor. Of course, the thing about kidney exchange is that each pair of people gives one kidney and receives one kidney. It is very egalitarian. I think kidney exchange is a good place to combat this notion that transplantation is like trafficking,” he notes.
—Notions, perceptions are very important. Many people think of “exchange” as the exchange of securities in the stock market.
“That's right, but not every exchange involves money. One of the discussions about money in the world that is taking place in the European Union at the moment is about payment to blood plasma donors. In the EU, only Germany, Austria, the Czech Republic and Hungary pay blood plasma donors. And those are the only EU countries that have as much blood plasma as they need. The others have to import everything, and they do it from the United States. The United States is the Saudi Arabia of blood plasma (…) The World Health Organization says that plasma must be obtained in each country, and from unpaid donors. You have to be self-sufficient... an economist finds that a little funny. Blood is a matter of life and death. “When there is a pandemic, we do not tell countries that they must be self-sufficient [in vaccines].”
—When we talk about these exchanges of blood plasma and kidneys, school choice systems, we are talking about the same idea: coincident or paired markets. But the concept of the market has been so questioned, especially by some political groups, for so long...
"It's true. Now, kidney exchange is special because money doesn't change hands. Money changes hands to get medical care, you have to pay doctors, nurses and hospitals. But we are not talking about buying kidneys from donors, but rather that, at the patient level, each pair receives a kidney and donates a kidney. It is radically egalitarian. Many people who think about markets may not think of it as a market, but I think that's a mistake. Many markets are not just about money… we would worry much less about markets if income and wealth inequality did not exist. “What worries us about markets is that some people are poor and some people are rich, and markets seem like a way to give the rich an advantage.”
“There is no doubt that being rich is better than being poor. The real question is what do we do to alleviate poverty. Making it invisible is not the same as alleviating it. One of the reasons I think many countries don't allow blood and plasma donors to be paid is because they don't like the way that looks. It reminds them that some people would like to get some money and would donate blood for it.”


Apparently, according to the caption, I'm "affable and smiling" (although not in this picture:)
Saturday, December 23, 2023
Market design: some press accounts in Chile
Wednesday, December 20, 2023